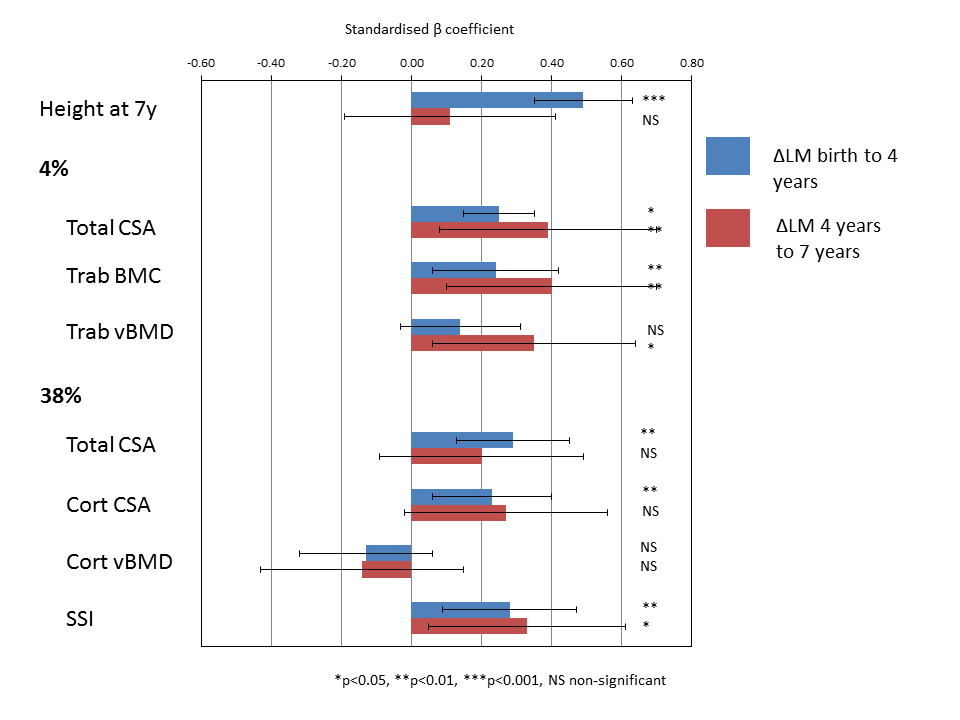
Using cohorts such as the Southampton Women’s Survey, the Norwegian Fit Futures study, the Helsinki Cohort Study and the Generation XXI birth cohort in Portugal, we have demonstrated important associations between trajectories of early growth and bone health in later childhood and adulthood. In the Southampton Women’s Survey, growth in lean mass, adjusted for change in fat mass, from birth-7 years, was associated with pQCT measures of bone more robustly than were measures of fat mass [Figure]. The greater role for the accrual of lean mass compared with fat mass on indices of bone density was also apparent in the Tromso Fit Futures cohort with the pattern of growth (persistent compared intermittent gain since birth), associated with greater bone mineral accrual in the Generation XXI birth cohort. Work from the Helsinki Cohort has demonstrated characteristics of growth in childhood associated with greater BMC and reduced fracture risk in adulthood. In ongoing work we are assessing growth trajectories in the Southampton Women’s Survey in relation to bone mass and body composition assessed at age 11-12 years, and planned at age 17 years, and to elucidate the relationships between early growth, the modifying effect of the pubertal transition on later bone mass, size, geometry, microarchitecture (from high resolution pQCT) and the role of body composition. We will complement this work with studies using very large cohorts including UK Biobank and the Spanish SIDIAP dataset.